Clinical Neuropsychotherapy
In November 2016 I ventured to Sydney, Australia to complete the coursework to become a Certified Clinical Neuropsychotherapy Practitioner. This class provided the skeleton that I needed to integrate the knowledge that I had acquired over the years. Sitting right in front of him, as I actively listened to Professor Pieter Rossouw I felt that the content of the training was providing me a “coherent narrative” (Siegel, 2012) for my academic, clinical and professional training along with what I have learned to know as my emerging vocation.
Early on during my graduate work at Santa Clara University, I had wondered if I should continue onto a doctorate program that would allow me to develop my own theory and run my own research projects. After seeking the advice of my professors, I decided that I would strive to be a ‘knowledge integrator’ rather than investing my time in creating my own. It is in situations like this that my engineering way of thinking kicks in and directs me to focus on efficiency. I figured that if I could consume the fruits of the findings of hundreds of clinicians and researchers from all over the world, I would be able to develop a more integrative approach in the least amount of time to help my clients to live a relational, resilient, and fulfilled life.

Practical, Integrative, and Multidisciplinary
My clinical neuropsychotherapy training experience gave me the template to bring together the many multidisciplinary areas of knowledge that I had been following and attempting to integrate since my encounter with Harry Harlow’s research with rhesus monkeys (Harlow, 1958) at the Esalen Institute in 2002, resulting in the development of what I call the People Systems Relational & Neuro-Developmental Approach to Human Dynamics by bringing together the latest research and clinical findings from diverse fields of knowledge such as attachment theory (Bowlby, 1969; Bowlby, 1973; Bowlby, 1980; Bowlby, 1988; Ainsworth et al,. 1978); affective and developmental neuroscience (Tronick, 2007; Porges, 2011; Panksepp, 1998); affect regulation theory (Schore, 2012); emotional intelligence (Goleman, 1995); human motivation (e.g., self-determination theory: Deci & Ryan, 2008; Ryan & Deci, 2000); behavioral epigenetics (Baylin, 2013; Cozolino, 2014; Meaney, 2010); reflective functioning (Slade, 2005); infant mental health and developmental science of early childhood (Gold, 2017); mentalization (Fonagy et al., 1991); complex and developmental trauma (Ogden et al., 2006; Levine, 2010; Ogden & Fisher, 2015; van der Kolk, 2015); and interpersonal neurobiology (Siegel, 2012) with my clinical training in object relations therapy (Greenberg & Mitchell, 1983; Winnicott, 1960; Winnicott, 1965; Winnicott, 1971, Winnicott, 1986); along with the critical influence by the child and family systems work of Daniel Hughes (Becker-Weidman & Hughes, 2008; Hughes, 2006; Hughes, 2009; Hughes, 2011; Hughes & Baylin, 2012; Baylin & Hughes, 2016), my clinical group consultation with Teri Quatman (Quatman, 2015);and the mentorship and clinical consultation that I have received from Michael Axelman (Axelman & Shapiro, 2012) since 2011.
While I had been ready to share my approach for quite sometime, I had not found the right clinical & theoretical framework until I attended the clinical neuropsychotherapy certification training in Sydney in November 2016 and completed all certification requirements.

In Neuropsychotherapy: Theoretical underpinnings and clinical applications, Professor Peter Rossouw, president of the International Association of Clinical Neuropsychotherapy, quotes the work of Klaus Grawe (Grawe, 2007) when providing his thoughts about what makes the field of neuropsychotherapy unique:
“The uniqueness of neuropsychotherapy is its focus on the neural processes that underlie human responses – memory, sensations, emotions, thoughts, behaviors and interactions. It underpins a sound recognition of the neural processes that provide a window into the essence of wellness and psychopathology and provides guidelines, generated through neuroscience, towards addressing dysfunctions” (Rossouw, 2014, p. 2).
Matthew Dahlitz, editor in chief of The Neuropsychotherapist, managing director of the Neuropsychotherapy Institute, and chief editor of the International Journal of Neuropsychotherapy also quotes the work of Klaus Grawe (Grawe, 2007) as he elaborated on the approach of neuropsychotherapy:
“The neuropsychotherapist aims from a ‘bottom-up’ perspective to understand the neural underpinnings of pathology through the lens of life experience and the meeting of basic needs, and to apply specific therapies to change this neurobiology toward a satisfaction of those basic needs” (Dahlitz, 2013, p. 82).

Why does all of this matter?
As I saw a powerpoint slide that Professor Rossouw displayed at the beginning of my neuropsychotherapy certification in Sydney, I started to realize that what he was saying was addressing several frustrations that I had been wrestling with since I began my clinical training in working with children. These frustrations had to do with how the medical model, in its effort to provide a diagnosis to the child, ends up missing the story that the child is trying to communicate through the symptoms being displayed. In addition, due to the reductionistic nature of the medical model, and the nature of child development which results in the child’s inability to use language to communicate how they feel, children end up with multiple diagnoses which at times point to different treatment approaches. What I realized is that regardless of the symptoms, the source of such symptoms is due to disregulation of the person’s stress response system.
What I was learning from the training was ‘giving words’ to the frustrations that I had experienced. The message was that the treatment was the same, regardless of the symptoms because the source of the disregulation was the same.
As the certification proceeded, we learned that the symptoms which lead people to present as isolating, avoidant, anxious, sad, compulsive, manipulative, angry, selfish, etc. happen when the person’s fear centers are upregulated – resulting in the person not feeling safe. A person can’t love, relate, have empathy for others and be part of a family or community if the person does not feel safe. And this sense of safety is not a thought or an emotion. It is visceral. It is a discomfort that is felt in the body, but for which the person has no language to express. The quickest way to help the person acquire a sense of neuroceptive safety (Porges, 2011) is through interventions from people with whom the person has an attachment bond.

The traditional treatment is to try to convince the person to use coping skills or to change their ways in order to become 'better adjusted' without exploring the emotional dynamics that are related to the behaviors that are getting the person in trouble. Parents might give consequences to their children, and at times criticize the negative behavior as unacceptable. I had learned through my clinical training that these approaches backfire because they ignore that the neural networks that are responsible for this behavior are pretty well developed. Like a muscle that gets worked every day at the gym, the neural networks that are at the source of these behaviors are very robust. Directly trying to change them will most likely turn into an argument with the child. The analogy that I give parents is that nobody would ever try to stop a wild horse by standing on its way. The reason why these networks are so strong is because we feel neurological pleasure through the discharge of dopamine even when the behaviors that we are carrying out are causing us difficulty. The behaviors are defensive, and any type of defensive stance has an important purpose if we understand the story that the person’s behavior is trying to communicate. The maladaptive, defensive, inappropriate behavior is fulfilling a longstanding narrative – what I call a primitive narrative. We can’t help the person if we don’t understand the primitive narrative that is responsible for the negative behavior.
In order to understand the primitive narrative, we have to first ensure the person feels safe at a visceral level. We then have to join with his internal experience so that we can feel what is it like to be driven to carry out such primitive narrative. This is important because the entire healing process is based on empathy. My experience is that it is almost impossible to give someone a label that points to an annoying behavior and at the same time be empathic. The treatment goal is to join with the client, and then assist the client in developing an alternative narrative, what I call a Relational Neuro-Narrative™ – a way of looking at oneself, others and the future that eventually results in a competing set of neural networks which initially will look very small in comparison to the very well developed networks analogous to the primitive narrative.
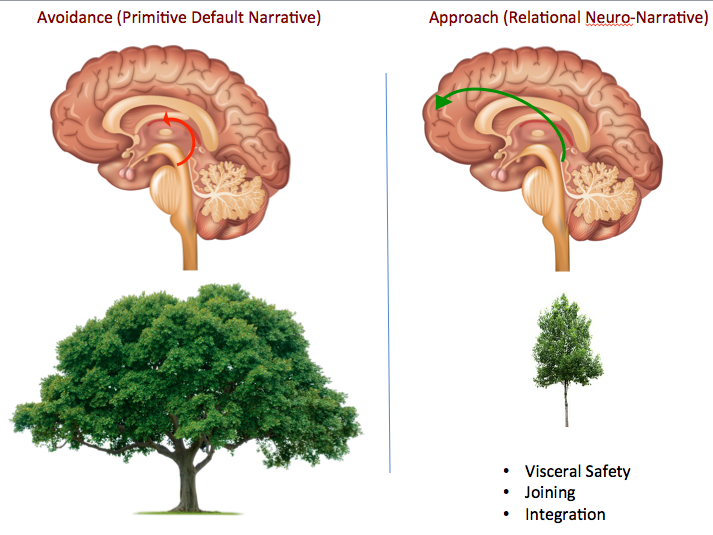
By the time my certification training was over, I had in my mind a visual which I now use with my clients. On the left side, I am using a big tree with many branches to represent the well-developed primitive narrative. This is the result of a person that can't move forward in life because is unable to use the executive functioning capabilities that reside in the prefrontal cortex since when the amygdala is disregulated, the person can’t think. As the client feels safe, a series of neurochemical processes result in the soothing of the amygdala, which in turn allows the connections from the limbic system to the prefrontal cortex to become stronger. I represent this by the small tree on the right side of the diagram. The safer the person feels, and the more I am able to join with the person’s disregulated experience, the more motivated the client will be to try new activities that will slowly nourish the alternative Relational Neuro-Narrative™. The key is that the therapist should focus on ensuring the client feels safe through unconditional positive regard, empathy, and acceptance in order to assist the development of the healthier behaviors, which will transition the client into a more resilient and thriving lifestyle.
References
- Ainsworth, M. S., Blehar, M. C., Waters, E., & Wall, S. (1978). Patterns of attachment: A psychological study of the strange situation. Oxford, England: Lawrence Erlbaum.
- Axelman, M. J., & Shapiro, J. L. (2012). An introduction to child counseling and psychotherapy: A relational developmental approach. Unpublished Manuscript.
- Baylin, J. (2013). Behavioral Epigenetics & Attachment. The Neuropsychotherapist, 3, 68-79.
- Baylin, J. & Hughes, D. A. (2016). The neurobiology of attachment focused therapy: Enhancing connection and trust in the treatment of children and adolescents (Norton Series on Interpersonal Neurobiology). WW Norton & Company.
- Becker-Weidman, A., & Hughes, D. (2008). Dyadic developmental psychotherapy: an evidence-based treatment for children with complex trauma and disorders of attachment. Child & Family Social Work, 13(3), 329-337.
- Bowlby, J. (1969). Attachment and loss. Vol. 1: Attachment. New York: Basic Books.
- Bowlby, J. (1973). Attachment and loss. Vol. 2: Separation. New York: Basic Books.
- Bowlby, J. (1980). Attachment and loss. Vol. 3: Loss, sadness, and depression. New York, NY, US: Basic Books.
- Bowlby, J. (1988). A secure base: Parent-child attachment and healthy human development. New York, NY, US: Basic Books.
- Cozolino, L. (2014). Experience-dependent plasticity: The science of epigenetics. The Neuropsychotherapist. 1 (5) Apr-Jun 2014, 40-53.
- Dahlitz, M. (2013). Integrating two theoretical approaches: Neuropsychotherapy & Coherence Therapy. The Neuropsychotherapist, 3: 81-89.
- Deci, E. L., & Ryan, R. M. (2008). Self-determination theory: A macrotheory of human motivation, development, and health. Canadian psychology/Psychologie canadienne, 49(3), 182.
- Fonagy, P., Steele, M., Steele, H., Moran, G. S., & Higgitt, A. C. (1991). The capacity for understanding mental states: The reflective self in parent and child and its significance for security of attachment. Infant mental health journal, 12(3), 201-218.
- Greenberg, A., & Mitchell, S. (1983). Object relations in psychoanalytic theory. Harvard University Press.
- Gold, C. M. (2017). The developmental science of early childhood: Clinical applications of infant mental health concepts from infance through adolescence. W. W. Norton & Company.
- Goleman, D. P. (1995). Emotional intelligence: Why it can matter more than IQ for character, health and lifelong achievement. Bantam Books.
- Grawe, K. (2007). Neuropsychotherapy: How the neurosciences inform effective psychotherapy. Lawrence Erlbaum Associates Publishers.
- Harlow, H. F. (1958). The nature of love. American psychologist, 13(12), 673.
- Hughes, D. A. (2006). Building the bonds of attachment: Awakening love in deeply troubled children. Jason Aronson.
- Hughes, D. A. (2009). Attachment-focused parenting: Effective strategies to care for children. WW Norton & Company.
- Hughes, D. A. (2011). Attachment-focused family therapy workbook. WW Norton & Company.
- Hughes, D. A., & Baylin, J. (2012). Brain-Based Parenting: The Neuroscience of Caregiving for Healthy Attachment (Norton Series on Interpersonal Neurobiology). WW Norton & Company.
- Levine, P. A. (2010). In an unspoken voice: How the body releases trauma and restores goodness. North Atlantic Books.
- Meaney, M. J. (2010). Epigenetics and the biological definition of gene× environment interactions. Child development, 81(1), 41-79.
- Ogden, P., Minton, K., & Pain, C. (2006). Trauma and the body: A sensorimotor approach to psychotherapy (norton series on interpersonal neurobiology). WW Norton & Company.
- Ogden, P., & Fisher, J. (2015). Sensorimotor Psychotherapy: Interventions for Trauma and Attachment (Norton Series on Interpersonal Neurobiology). WW Norton & Company.
- Panksepp, J. (1998). Affective neuroscience: The foundations of human and animal emotions. Oxford University Press.
- Porges, S. W. (2011). The Polyvagal Theory: Neurophysiological Foundations of Emotions, Attachment, Communication, and Self-regulation (Norton Series on Interpersonal Neurobiology). WW Norton & Company.
- Quatman, T. (2015). Essential psychodynamic psychotherapy: an acquired art. Routledge.
- Rossouw, P. J. (2014). Neuropsychotherapy: Theoretical underpinnings and clinical applications. Brisbane, AUS: Mediros Pty Ltd.
- Ryan, R. M., & Deci, E. L. (2000). Self-determination theory and the facilitation of intrinsic motivation, social development, and well-being. American psychologist, 55(1), 68.
- Schore, A. N. (2012). The Science of the Art of Psychotherapy (Norton Series on Interpersonal Neurobiology). WW Norton & Company.
- Siegel, D. J. (2012). The developing mind, second edition: How relationships and the brain interact to shape who we are. Guilford Publications.
- Slade, A. (2005). Parental reflective functioning: An introduction. Attachment & human development, 7(3), 269-281.
- Tronick, E. (2007). The neurobehavioral and social-emotional development of infants and children. WW Norton & Company.
- van Der Kolk, B. (2015). The body keeps the score: Brain, mind, and body in the healing of trauma. Penguin Books.
- Winnicott, D. W. (1960). The theory of the parent-infant relationship. The International journal of psycho-analysis, 41, 585.
- Winnicott, D. W. (1965). The maturational process and the facilitating environment. International University Press.
- Winnicott, D. W. (1971). Playing and reality. Psychology Press.
- Winnicott, D. W. (1986). Home is where we start from: essays by a psychoanalyst, DW Winnicott. Penguin Books.